
Research Blog
How to Write a Case Report: An Easy, Step-by-step Guide to Writing a Clinical Case Report


I hope you enjoy reading this blog post.
Hello everyone! Welcome to our tutorial and a step-by-step guide on how to write a Case Report.
What is a Case Report or a Case Series? What does a case report mean?
While there’s not a single-standardized definition for what a case report or a case series is, it can be best described as a scientific publication focused on the description of an unexpected or unique disease presentation, clinical course or treatment strategy. By extension, a Case Series is a group of various similar cases. While there’s no hard consensus on the number of patients needed for a case series, a good rule of thumb is:
- 1 Patient: Case Report
- 2-4 Patients: Case Report or Case Series
- >4 Patients: Case Series
Are Case Series considered Cohort Studies?
Case series may accrue a large number of patients (well into the hundreds) but they lack a control group. On the other hand, cohorts and case control studies have a control group which is used to compare against using statistical analysis.
How do I know if my clinical case report is “publishable”? How do I do a literature review for a case report?
Before you invest your time into fully writing up the case, it’s important to determine its publishing potential. By FAR, the best way to determine this is by reviewing the literature. While it may seem daunting, this does not mean you’ll spend months sifting through hundreds or thousands of publications. Instead, follow our simple steps:
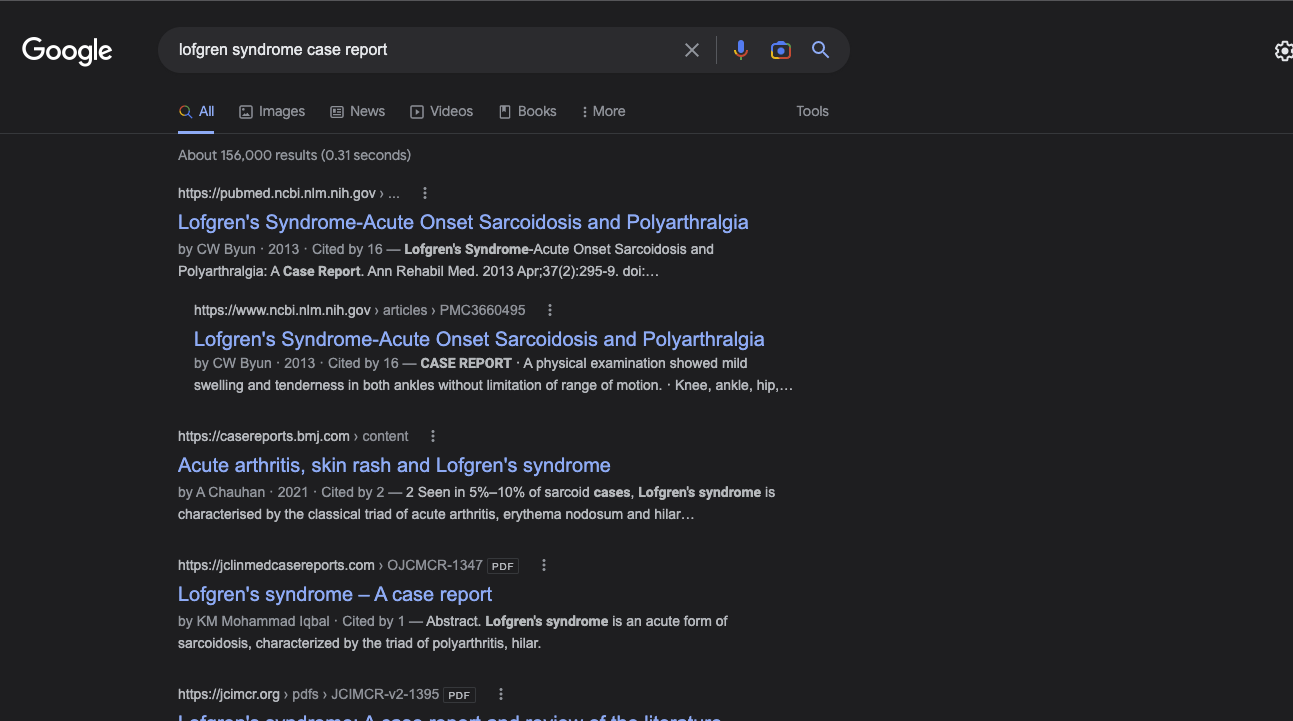
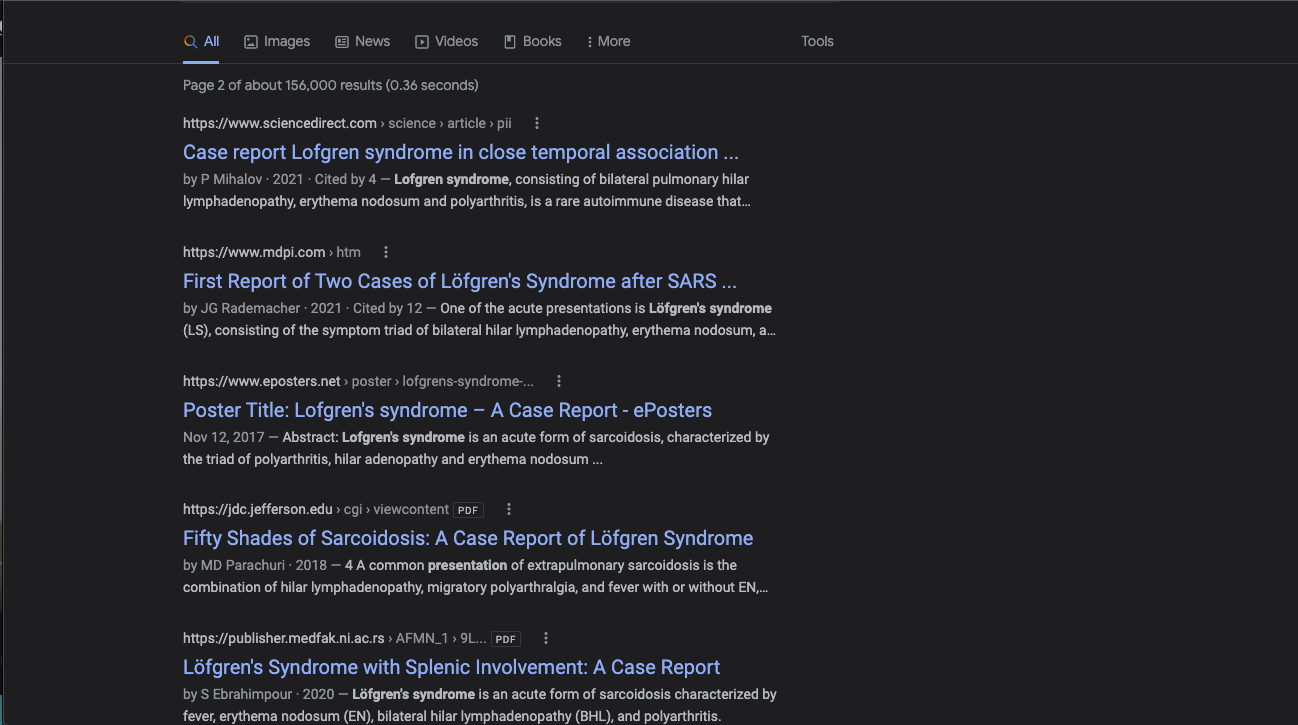
- Google your disease/case + case report. Go through the first page of results, how many of these links are actual publications? How many of these are links to PubMed?
- Go to PubMed and repeat the search. You can gauge the number of hits you get, use the filter -> case report or command/control + f “case report” to count how many of the results are case reports. Pay special attention to the year and journal in which they were published. Be careful that the PubMed filter is not always accurate. For a full guide on how to perform a literature review, check out our Comprehensive Research Course, from Idea to Publication.
- Go through the case reports you found and read them. How different or similar are they to your own case?
- Did my search for clinical case report yield case reports or large cohort/comparative studies? How many similar studies did I find? If you found only case reports and case series then your case may be “rare” enough to be publishable. On the other hand, if your search yielded cohort/comparative/case-control studies then it’s likely that there’s ample evidence and more complex studies available, reducing the attractiveness of your case report UNLESS there’s something truly unique about your case.
- If your search yielded case reports or series, which were more common? If you have only one patient and there are various case series with >10-20 patients, then your publication may not be as publishable UNLESS there’s something significantly different about your case. The same applies if you find 5-10 case reports about the same topic. Your case report has to bring something unique, something different that we don’t already know from existing literature.
- How different is your case from everything you read?
A similar search in PubMed yields 137 results, out of which probably not all are truly Lofgren Syndrome Case Reports and thus it’s likely viable.
This should be followed by an assessment of reported cases, noting similarities and differences between your case and reported literature.
What specialties publish Case Reports?
In theory, every specialty publishes case reports. However different specialties will have different interests in what a case report should include. For example, a case report for a radiology journal will have a different focus than if it was written for a surgical journal. For the former, readership and editors might find details related to radiologic findings to be more interesting than surgical pictures and vice versa.
Additionally, some specialties have dedicated journals to case reports. For example, urology has Journal of Endourology – Case Reports. For Surgery, there are journals such as the Journal of Surgical Case Reports that solely publish case reports.
What are the components of a Case Report?
Like most published literature, case reports follow a structure which typically consists of:
- Abstract
- Introduction
- Case Presentation
- Discussion
- Conclusion
Research Course
The research course will teach you how to take a research project from idea to publication and in which I will share my 3-year experience of clinical research in which I had over 100 publications and 80 presentations.
Are there “rules” or “guidelines” for Case Reports?
The CARE guidelines are generally regarded as the standard “checklist” for publishing a quality case report and some journals ask for the checklist to be submitted along with the manuscript. Here you can find more information about the CARE guidelines: https://www.care-statement.org/
How do I start writing a Case Report?
Once you’ve gauged the literature for the feasibility of publishing, you should gather all the possible case information. You can use the case reports you found as a guide as to what you’ll need, but in general, try to obtain data on:
- Accurate presentation, physical exam findings and relevant patient history.
- Lab values and imaging studies, when necessary, some diseases also benefit greatly from pathology slides.
- Treatment: specifics on duration of pharmacologic therapy, if it was surgical, nuanced description and pictures of the surgery.
- Follow-up results: For certain conditions, a longer follow-up is needed. You can gauge this from other published case reports.
- Patient satisfaction or measured outcomes. There is a plethora of scales that attempt to objectively measure subjective components such as functionality, pain and quality of life. Additionally, all specialties have their own internal scores used to assess severity and treatment usefulness such as the SPSS for benign prostatic hyperplasia, the EuroQoL quality of life score and so on.
Interested in learning more about literature search with examples from published literature?
Check out the Free Lessons of the Comprehensive Research Course
How do I write an Introduction for a Case Report?
Case report’s introductions are very similar in structure and purpose to any other published study. The aim of any introduction is to give background about the topic you are presenting. Typically, introductions have 3-4 paragraphs. For case reports, introductions might be 1-2 paragraphs or sometimes even a few lines based on the word limit allowed by the journal. Think of a funnel or an inverted triangle where you go from general/broad to specific. Your prior literature review should help you fill out the paragraphs.
The first paragraph will typically: describe the disease, etiology, and provide brief epidemiologic data in 2-3 sentences. This is usually followed by typical clinical presentations or other related findings/or treatments. In a broad sense, the first paragraph is a very general summary of the background of this condition.
The second paragraph will transition into setting the context as to why your case is important or different. Why there’s a gap or need for this case. Think of it as selling or pitching something. Depending on your case and its focus it will range from a rare presentation or findings to variations in treatments or procedures.
Lastly, your last paragraph is a brief, concise summary of what the report entails, usually something like
“We present a case report of X condition treated successfully with X technique and adequate outcomes”.
When writing your first introduction it’s easy to get overly excited and extend too much. It’s important to stay focused and on-topic. A good rule of thumb is to keep introductions at around 300 words.
Another important point to keep in mind is the context of your readership and make it understandable for a broad readership.
Let’s start with a short introduction that condenses all the above-mentioned points in a single paragraph. The following case report “Dangerous mistake: an accidental caffeine overdose” published in BMJ Case Reports will be our first example.
Example 1 Case Report Introduction:
Caffeine intoxication
Caffeine intoxication
1st Paragraph
“This case illustrates the life-threatening consequences, such as malignant cardiac arrhythmias, of severe caffeine poisoning, which is a rare event. Also, it highlights the risk of accidental caffeine overdose associated with sports practice, which can be related, not only, to the difficulty in measuring small portions, but also due to unclear consumer’s instructions.”
As we go through examples, you’ll see the various ways introductions or backgrounds can be written to serve specific purposes. In this case, the brief background/introduction is centered on “justifying” the importance of the case.
Abstracted from: Andrade A, Sousa C, Pedro M, Fernandes M. Dangerous mistake: an accidental caffeine overdose. BMJ Case Rep. 2018;2018:bcr2018224185. Published 2018 Jun 8. doi:10.1136/bcr-2018-224185
In this other example published in Annals of Medicine and Surgery we can see how the 3-paragraph structure is a great starting point but is not a rule per se and can be shaped or wrapped into the authors preference.
Example 2 Case Report Introduction:
Gallstone Ileus
Gallstone Ileus
1st paragraph
“A gallstone ileus is a mechanical intestinal obstruction caused by a gallstone impaction within the gastrointestinal tract. It mainly occurs following the formation of a cholecystoenteric fistula, most commonly in the duodenum and secondly in the colon. A cholecystocolonic fistula (CCF) is a late complication of repeated episodes of chronic inflammation of the…Impaction of a gallstone in the sigmoid colon causing a large bowel obstruction is rare and it’s usually at the sites of previous inflammation or colonic disease”
In this excerpt abstracted from the article, notice how it plays the role of the 1st and second paragraph by introducing gallstone ileus and mentioning how fistulation between the gallbladder and colon are rarer (and later ties down this fact by mentioning that there are only 250 reported cases).
2nd Paragraph
“Here we present a case of a 49-year-old female patient presenting with abdominal pain and bowel obstruction due to a gallstone impaction on the sigmoid colon due to a CCF. No more than 250 cases have been reported; a review of the literature of this rare condition is also revised. The work has been reported in line with the SCARE criteria”
Since the previous paragraph covered the essential functions of the typical paragraphs 1 and 2, in this example, paragraph 2 presents a summary of what will be presented (which is typically paragraph 3)
Alternatively, introductions can be lengthened a bit if needed, as in this example from “Balo’s Concentric Sclerosis with monophasic course: A report of 2 cases” published in Annals of Medicine and Surgery
Watch our video, “How to Write & Publish Case Reports” to learn exactly how to successfully create and publish a high-quality case report:
Example 3 Case Report Introduction:
Balo’s Concentric Sclerosis
Balo’s Concentric Sclerosis
1st Paragraph
“Balo’s Concentric Sclerosis (BCS) is a rare demyelinating disease considered a variant of multiple sclerosis (MS). It presents acutely with focal neurological deterioration. Magnetic Resonance Imaging (MRI) is the diagnostic modality, which usually reveals concentric lamella in cerebral white matter with “onion-like” lesions…”
This paragraph introduces BCS and expands on its history and first reported case, which could arguably be removed or shortened. Notice the brief mention of presentation, findings and prognosis.
2nd Paragraph
“BCS often affects young adults and three different clinical courses have been described; including an acute and self-limiting, remittingrelapsing variant and rapidly progressive primary disease. These last 2’s clinical and radiological characteristics appear to be more strongly related to MS. BCS usually courses with solitary lesions, which may persist for years. These lesions may regress and resemble typical demyelinating plaques.”
Contrasting to prior examples, notice how the authors are still covering the same topic, BCS, however, they are diving deeper on the 3 typical behaviors of the disease and their associated prognosis as well as diagnosis.
3rd Paragraph
“BCS is a variant of MS or separate entity. Prior authors have hypothesized increased risk of progression to MS when multiple bands and/or oligoclonal bands are found. In this report we describe two patients presenting at an academic institution with BCS, which presented with a monophasic course, and characteristic Balo lesions in MRI that disappeared during a long term follow up.”
In this paragraph, notice how authors “sell” the value of this series of cases. Prior literature suggests there’s a risk of progression in certain presentations but they present 2 cases with no progression.
Abstracted from: Martinez HR, Rodriguez-Gonzalez IC, Escamilla-Garza JM, Figueroa-Sanchez JA, Garcia-Aleman AC, Hinojosa-Gonzalez DE. Balo’s Concentric Sclerosis with monophasic course: A report of 2 cases. Ann Med Surg (Lond). 2021;68:102602. Published 2021 Jul 28.
Further reading/examples:
First human face allograft: early report
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(06)68935-6/fulltext
Metastatic Cutaneous Apocrine Adenocarcinoma Treated With a Combination of Pertuzumab-Based Targeted Therapy and Taxane Chemotherapy
A Case Report
https://jamanetwork.com/journals/jamadermatology/fullarticle/2436320
Deformation of cranioplasty titanium mesh in a paediatric patient following head trauma
https://pubmed.ncbi.nlm.nih.gov/31189547
How to find research positions in the US
This live and interactive session + recorded lessons will go over the details of finding research positions in the US.
How do I write up the case presentation?
As mentioned previously, the best guide on the specifics of the case you’re trying to write is the prior case reports published.
The typical main components that serve as the foundation for any case report regardless of the focus are:
- Accurate presentation, physical exam findings and relevant patient history.
- Lab values and imaging studies, when necessary, some diseases also benefit greatly from pathology slides.
- Treatment: specifics on duration of pharmacologic therapy, if it was surgical, surgical technique along with intraoperative photos.
- Follow-up results: For certain conditions, a longer follow-up is needed, you can gauge this from other published case reports.
- Patient satisfaction or outcomes. For most pathologies, there are verified classification scores and other scales that are applicable to objectively measure outcomes that may be subjective to a degree. As examples, Euro QoL measures quality of life in general, USSQ for ureteral stent wearers, mini-mental for cognitive assessment and so on. Additionally, patient input per se may be used in the case report if they have an objective assessment of their own outcomes or satisfaction.
Example 1:
Caffeine Overdose
Caffeine Overdose
“A 32-year-old woman with no significant medical and family history presented to the local emergency department (ED) referring malaise, anxiety, dizziness and nausea. Symptoms like chest pain, syncope, palpitations or fever were denied. The initial physical examination at triage revealed a Glasgow Coma Scale (GCS) of 15, a respiratory rate of 19 breaths/min, 100% oxygen saturation on room air, blood pressure of 112/70mm Hg, pulse of 80 beats/min and had a normal tympanic temperature. Also, the blood sugar was 147mg/dL. After observation, the patient had an episode of presyncope followed by agitation and vomiting. At this point, the patient was pale and sweaty with a GCS of 11 (eye opening: 4; verbal response: 2; motor response: 5), blood pressure of 115/75mm Hg, tachycardia (160 beats/min) and 99% oxygen saturation on room air…”
It is always best to start with presentation and past relevant history. However, it’s important to keep the context of the patient and the journal being submitted to in mind. For example, in this case in the emergency department, blood pressure, heart rate, saturation, GCS are all very important, whereas in a pathology focused case report they might not.
“The initial group of complementary exams was:
► Electrocardiogram (figures 2 and 3) showing a broad QRS polymorphic tachycardia.
► Arterial blood gas showed a metabolic acidosis with pH of 7.296 (7.35–7.45), pCO2 of 29.9mm Hg, pO2 of 117mm Hg, HCO3 of 16.1mmol/L (22–26) and severe lactataemia with serum lactate level of 5.3mmol/L (0.5–1.6).
► Prominent laboratory findings included mild leucocytosis of 13.50×109 /l (4.0–10.0) with 68.3% neutrophils, hyperglycaemia of 254mg/dL (70–105), hypocalcaemia of 2.5mmol/L (3.5–5.1) and hypophosphataemia of 1.8mg/dL (2.3–4.7). Magnesium and calcium serum values were within normal range as well as thyroid, renal and liver function tests. Urinalysis was positive for ketones and glucose and negative for cocaine and opioid drugs.”
Work up should follow on the premises set during the initial presentation and case history. While some patients may have undergone a plethora of tests, try to focus on the ones relevant to the presentation. For example, in this case, treating physicians were working up a possible intoxication as a main diagnosis, in such case if the patient underwent additional unrelated testing (as a ridiculous example, a colonoscopy) it may be better to omit to keep the sections short and concise.
“The supportive treatment, including intravenous fluids, propranolol, potassium and phosphorus supplementations, stabilised the patient’s clinical status. No activated charcoal was administered as the medical team was unaware of a dietary product ingestion during the initial evaluation. After 48hours of observation in our intermediate care unit, the patient was transferred to the ward, since she only had a asymptomatic sinus tachycardia (maximum of 120 beats/min), with other vital signs remaining stable and normal serum pH, lactate and glucose levels.”
Treatment should follow along the narrative and be focused on relevant strategies for the underlying disease.
“The patient remained in our intermediate care unit for 2 days, with normal level of
Outcomes and follow-up are one of the most important sections of the case report, make
consciousness maintained, normalisation of arterial blood gas values and no recurrence of presyncope episodes. However, she had persistent sinus tachycardia and, for this reason, was submitted to a 3-day course of 30 mg/day oral propranolol with heart rate control. The patient remained clinically stable and 5 days later was discharged asymptomatic referred to internal medicine follow-up… Six months after the episode, at follow-up evaluation, the patient remained asymptomatic.”
sure you include relevant systems/scores and any lingering symptom.
Abstracted from:Andrade A, Sousa C, Pedro M, Fernandes M. Dangerous mistake: an accidental caffeine overdose. BMJ Case Rep. 2018;2018:bcr2018224185. Published 2018 Jun 8. doi:10.1136/bcr-2018-224185
Example 2:
Gallstone Ileus/Cholecystocolonic Fistula
Gallstone Ileus/Cholecystocolonic Fistula
In contrast with the prior example, this case is much more straightforward as the focus is more on the surgical treatment rather than addressing a multisystemic unknown disease.
“A 49-year-old female patient was admitted to the hospital with severe abdominal pain, nausea, vomiting, and constipation following a 3- day history of colicky middle abdominal pain. The patient had no relevant medical history. On examination the patient was hemodynamically stable and afebrile. Physical examination revealed abdominal distension with decreased bowel movements to auscultation accompanied by diffuse tenderness to superficial and deep palpation and a tympanic colonic margin to percussion…”
Presentation and relevant history. Notice how it’s focused on relevant aspects to the scenario in which the patient presented (i.e abdominal pain in the E.R. where hemodynamical stability is important vs a case of a rare condition in an outpatient clinic where it might not be as important)
“Laboratories showed a normal hemoglobin, WBC of 6.7 × 10ˆ 10 and no alterations in liver enzymes, except for an elevation in GGT, with a value of 226UL. Simple abdominal radiographs were performed, observing dilated loops of the small bowel, and no signs of gas in the rectum. A CT was ordered, revealing a 3 × 2 cm calcified mass in the sigmoid colon, suggestive of a gallstone, with associated enlargement of the surrounding intestinal wall, with stranding pericolonic fat and signs of diverticular disease…”
Laboratory, imaging and other work-up. Same concept as above, focused on relevant findings for this patient’s scenario.
“The patient underwent an exploratory laparotomy, and after the abdominal cavity was exposed, signs of dilation of the small intestinal loops became evident. An intraluminal, solid, non-mobile mass was found in the sigmoid colon. An enterolithotomy was performed, and a 4 × 4 cm gallstone was extracted without complications, performing a primary transverse closure of the colon. A fistulous track was observed between the gallbladder and the hepatic flexure of the colon…The patient had an adequate postoperative outcome, referring only moderate pain during the first day. Oral intake was reintroduced on the fourth day, without further complications. On the fifth POD the patient was discharged home, with good oral intake and with norma levacuations. “
Treatment and postoperative course. Since this is a surgical-focused case report, operative technique and a thorough description of the procedure are highly encouraged.
“On a 8 month-follow up, the patient is doing well with no biliary symptoms.”
Follow-up.

Example image from the case
Abstracted from: Mauricio GU, David Eugenio HG, Enrique QF. Gallstone ileus of the sigmoid colon caused by cholecystocolonic fistula: A case report. Ann Med Surg (Lond). 2018;31:25-28. Published 2018 Jun 6. doi:10.1016/j.amsu.2018.06.001
Example 3:
Balo’s Concentric Sclerosis
Balo’s Concentric Sclerosis
Case 1: “A 44-year-old man presented to the emergency room in September 2010 with sudden onset of dysarthria and dysgraphia. No history of cerebrovascular risk factors, relevant family history, past surgical or medical history as well as allergies were reported by the patient.”
Case 2: “A 25-year-old female without past family or medical history presented to the emergency room with left sided hemiparesis and left facial palsy in September 2020… the neurological examination revealed in the upper and lower left limbs weakness 2/5 in proximal and distal limb sectors, Hoffman and Trommer ¨ signs in the left side without Babinski response…”
Case 2: “A 25-year-old female without past family or medical history presented to the emergency room with left sided hemiparesis and left facial palsy in September 2020… the neurological examination revealed in the upper and lower left limbs weakness 2/5 in proximal and distal limb sectors, Hoffman and Trommer ¨ signs in the left side without Babinski response…”
Presentation and history.
Case 1: “An enhanced MRI showed a periventricular concentric demyelinating lesion in left periventricular area (Fig. 1A and B). Clinical and imagining findings raised suspicion for isolated MS clinical syndrome. A lumbar puncture revealed one OCB, 3 mononuclear cells and normal proteins in CSF. Somatosensorial evoked potentials were compatible with demyelinating disease. “
Case 2: “Stroke protocol MRI revelaed a right sided periventricular concentric demyelinating lesion with a concentric ring pattern that showed enhancement after endovenous contrast injection…The CSF showed normal proteins, no leukocytes and the OCB were negative. “
Work-up.
Case 1: “The patient received IV methylprednisolone (1000 mg/day for 5 days) showing clinical improvement and was discharged 5 days later without any neurological deficit. His neurologist prescribed interferon, once a week subcutaneously that was suspended one month later due to side effects. Case reassessment from a neurologist consulted for a second opinion suggested BCS. “
Case 2: “The diagnosis of BCS was established and the patient received IV methylprednisolone. (1000 mg/day for 5 days) and a remarkable clinical improvement was observed and one week later the patient was discharged.
“
Treatment.
Case 1: “The patient has remained asymptomatic and 10 years later (September 2020). Follow-up MRI revealed small gliosis in the left periventricular area.”
Case 2:
“She remains asymptomatic eight months after diagnosis.
“
Follow-up.
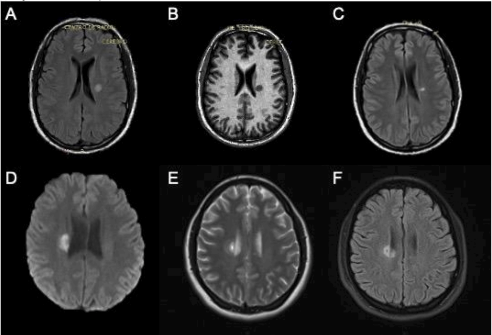
Images from the case
Abstracted from: Martinez HR, Rodriguez-Gonzalez IC, Escamilla-Garza JM, Figueroa-Sanchez JA, Garcia-Aleman AC, Hinojosa-Gonzalez DE. Balo’s Concentric Sclerosis with monophasic course: A report of 2 cases. Ann Med Surg (Lond). 2021;68:102602. Published 2021 Jul 28.
Further reading/examples:
First human face allograft: early report
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(06)68935-6/fulltext
Metastatic Cutaneous Apocrine Adenocarcinoma Treated With a Combination of Pertuzumab-Based Targeted Therapy and Taxane Chemotherapy
A Case Report
https://jamanetwork.com/journals/jamadermatology/fullarticle/2436320
Deformation of cranioplasty titanium mesh in a paediatric patient following head trauma
https://pubmed.ncbi.nlm.nih.gov/3118954

How do I write a Discussion for a Case Report?
The discussion is the section where the focus should be comparing and contrasting your findings to the prior published case reports. There are various ways to go about this and generally all are correct. You can start with a one-liner similar to the last paragraph or your introduction or a brief re-introduction of the disease.
During the discussion it’s important to address:
- Similarities and differences to prior published cases in both treatment and outcomes.
- Ponder/extrapolate on why or how those differences might impact selected treatment or outcomes. Open to further discussion such as using techniques in low-resource settings or similar.
- Emphasis on how your case is different and how your treatment or presentation “adds” to the literature.
- Wrap to a “key takeaway” which can be related to presentation, diagnosis, management or follow-up.
Some authors choose to summarize a study or 2 per paragraph and directly compare those findings to their own study while others prefer to provide a general overview without fixating on any one study specifically.
Example 1 Case Report Discussion:
Gallstone Ileus
Gallstone Ileus
In this example, authors contrast their case and treatment to that of published literature, sometimes addressing changes in standardized or expected treatment.
“The exact etiology of CCF secondary to gallstone disease may vary. Glenn et al. in their study of a few more than a hundred bilioenteric fistulas, stated that acute inflammation of the gallbladder with obstruction of the cystic duct allows adhesion of the gallbladder to the contiguous organs. This promotes ulceration and ischaemia of the wall of the gallbladder and the adjacent organs, creating an anomalous communication between them…”
Reintroduction of the general context of the case is a great way to set up the discussion which should center on discussing similarities and differences.
“Clinical signs of CCF are usually minimal, and preoperative diagnosis of CCF is rare and only considered in 7.9% of all CCF, therefore the diagnosis is often made intraoperatively. Signs and symptoms of a CCF may vary, as it often presents with abdominal pain, nausea, vomit, diarrhea, weight loss, and malabsorption…”
Clinical presentation as reported in the literature is provided to better assess and contrast how this case was different or similar from the reported literature.
“Gallstone impaction occurs most frequently in the small intestine, followed by the colon in 8% of the cases. In the vast majority of patients presenting with CCF and biliary ileus, the stone is located at the sigmoid colon. The size of the gallstone is presumed to determine whether and where a migrated stone will impact. Small and mid-sized stones are thought to pass through the entire colon, thus being easily expelled through stools; whereas gallstones over 2.5 cm in diameter may cause colonic obstruction at the sigmoid colon…”
Common impaction locations, again, providing in-depth context. As previously mentioned, it’s important to scrutinize the presented case against published literature as much as possible.
“Our patient had diverticular disease and a gallstone of 4 cm, predisposing it to impact at this point. Misdiagnosis is common and it also carries a significant rate of complications with a mortality rate ranging from 12% to 27% in most series reported. Preoperatively diagnosis is therefore critical to improve morbidity, mortality and post-operative complications…”
Possible etiologies
“Treatment of CCF has changed through the years; traditional treatment during the early 80s suggested a ‘‘two-stage’’ procedure, performing a diverting colostomy. Nowadays, a ‘‘one-step’’ management has been considered the treatment of choice without significant complications being reported, versus doing only the enterolithotomy alone…”
Context for treatment and setting up discussion to analyze how frequent is the treatment provided by the authors.
“We opted to perform solely the enterolithotomy because the patient never experienced biliary colic or any other symptoms associated with gallbladder disease. We decided to correct only the occlusion during the laparotomy, as the surgical approach was less complicated, and it had a lower mortality rate. Simple enterolithotomy enthusiasts state the infrequency of recurrent gallstone ileus, and the rarity of complications directly related to a persistent gallbladder fistula, such as cholecystitis, cholangitis, malabsorption and carcinoma of the gallbladder. Also, when the occlusion is resolved, the possibility of spontaneous closure of the fistulous track is higher, leaving behind only a fibrous remnant.”
Rationale for treatment provided by the authors and outcomes.
Abstracted from:Mauricio GU, David Eugenio HG, Enrique QF. Gallstone ileus of the sigmoid colon caused by cholecystocolonic fistula: A case report. Ann Med Surg (Lond). 2018;31:25-28. Published 2018 Jun 6. doi:10.1016/j.amsu.2018.06.001
Example 2 Case Report Discussion:
Caffeine intoxication
Caffeine intoxication
For the previously analyzed case report on caffeine intoxication, authors opted for a more “review” type discussion where the discussion serves mostly as a summary of available literature on their presented topic.
“Caffeine (1,3,7-trimethylxanthine) is a natural product commonly found in foodstuffs, beverages and medicinal products. When relatively low doses of caffeine are consumed, severe side effects are uncommon. However, in recent years, larger amounts of caffeine have been added to energy drinks or taken as dietary supplements, such as anhydrous caffeine, for increasing endurance, concentration and athletic performance.”
This “review” style discussion begins with a reintroduction of the topic. Authors do this through a similar structure to the one we talked about for introductions. The inverted triangle starting from broad to specific.
“Normally, mild stimulation is obtained with a caffeine dosage of 0.05–0.2g. Even though fatal caffeine intoxication is rare, acute ingestion of >5g can be lethal… By blocking the adenosine receptors, at high doses, caffeine interacts with the sympathetic nervous system inducing prolonged and intensified beta-receptor activation with positive inotropic and chronotropic effects which can trigger arrhytmia. And in toxic doses, caffeine directly releases calcium from intracellular stores, which also may increase the susceptibility for arrhythmias. Symptoms of caffeine intoxication may include headache, fever, nausea, vomiting, tachycardia, dizziness, tinnitus, anxiety, irritability, insomnia and seizures…. Toxic levels of caffeine are also associated with severe hypokalaemia, hyperglycaemia, rhabdomyolysis, renal failure and hyperlactacidaemia…”
Authors then move to talk about specifically caffeine intoxication, its levels and severity as well as mechanism of symptomatology.
“Treatment of caffeine toxicity can vary on case-to-case basis. However, it should begin with careful and immediate assessment of the patient’s airway, breathing and circulation. Not only should non-invasive monitoring, like continuous cardiac monitoring, and fingerstick glucose level be rapidly obtained, but also intravenous access must be established. To prevent systemic effects of the caffeine metabolism, activated charcoal and intravenous lipid emulsion can be useful interventions. To address hypotension, intravenous fluid therapy with isotonic fluid should be initiated.Any patient with a haemodynamically unstable dysrhythmia should be treated by advanced cardiac life support protocols. In several published case reports, a combination of a shortacting beta-blocker (eg, esmolol, propranolol), procainamide or lidocaine with electrolyte correction successfully treated cardiac arrhytmias…”
Lastly, the authors address treatment and outcomes in their latter paragraphs. Given the rarity of caffeine intoxication, the discussion serves as an overall “primer” for the topic rather than a “classic” discussion where findings of the case are compared and contrasted to the literature.
Abstracted from:Andrade A, Sousa C, Pedro M, Fernandes M. Dangerous mistake: an accidental caffeine overdose. BMJ Case Rep. 2018;2018:bcr2018224185. Published 2018 Jun 8. doi:10.1136/bcr-2018-224185
Further reading/examples:
First human face allograft: early report
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(06)68935-6/fulltext
Metastatic Cutaneous Apocrine Adenocarcinoma Treated With a Combination of Pertuzumab-Based Targeted Therapy and Taxane Chemotherapy
A Case Report
https://jamanetwork.com/journals/jamadermatology/fullarticle/2436320
Deformation of cranioplasty titanium mesh in a paediatric patient following head trauma
https://pubmed.ncbi.nlm.nih.gov/31189547
How do I find a journal to publish my Case Report?
Journal selection should start by understanding that there are 2 types of journals. Case Report specific journals and Specialty journals. Case Report journals are typically open access, meaning there’s going to be an associated cost to publication. However, their acceptance criteria may be looser than a specialty journal. Even among these Case Report journals, there might be specialty focused journals such as for surgical cases, radiology cases and so on.
Google is a great way to find journals. For example, you can google “cardiology journals” or “cardiology case report journals” and browse results for a great starting point. You can then assess these journals’ author guidelines or prior issues for case reports. Additional input from mentors or friends may yield you other solid options.
When looking for journals be sure to check the costs associated with the journal, as these may reach thousands of dollars, however some countries or hospitals may have cost waivers.
Once you’ve found potential journals, it’s time to select a journal for submission. By far, the most important criteria are PubMed indexation and relative respect within its field. While indexation can be assessed on the journal website, respect can be assessed by asking a mentor or looking at the impact factor.
Some journals are predatory, and their main business model is taking your money to publish your cases. These journals have little to no academic value. Try looking at the Directory of Open Access Journals (DOAJ), Committee on Publication Ethics (COPE) or Open Access Scholarly Publishers Association (OASPA) for journals as they’re less likely to be predatory if they’re listed there. Additionally, look at each journal’s editorial board, if you find respected doctors from respected institutions it’s likely that it’s a good, non-predatory journal.
Additional resources to look for journals are Scopus and Scimagojr which may provide index lists. Some publishers such as Elsevier have “journal suggesters” in which you provide the abstract and an algorithm returns possible journals with an estimated match likelihood.
Google is a great way to find journals. For example, you can google “cardiology journals” or “cardiology case report journals” and browse results for a great starting point. You can then assess these journals’ author guidelines or prior issues for case reports. Additional input from mentors or friends may yield you other solid options.
When looking for journals be sure to check the costs associated with the journal, as these may reach thousands of dollars, however some countries or hospitals may have cost waivers.
Once you’ve found potential journals, it’s time to select a journal for submission. By far, the most important criteria are PubMed indexation and relative respect within its field. While indexation can be assessed on the journal website, respect can be assessed by asking a mentor or looking at the impact factor.
Some journals are predatory, and their main business model is taking your money to publish your cases. These journals have little to no academic value. Try looking at the Directory of Open Access Journals (DOAJ), Committee on Publication Ethics (COPE) or Open Access Scholarly Publishers Association (OASPA) for journals as they’re less likely to be predatory if they’re listed there. Additionally, look at each journal’s editorial board, if you find respected doctors from respected institutions it’s likely that it’s a good, non-predatory journal.
Additional resources to look for journals are Scopus and Scimagojr which may provide index lists. Some publishers such as Elsevier have “journal suggesters” in which you provide the abstract and an algorithm returns possible journals with an estimated match likelihood.
How much does it cost to publish a Case Report?
There’s no fixed cost to publishing. Most journals don’t have any submission or publishing fees. However, some open-access journals, such as those dedicated to publishing case reports typically have fees ranging from 500 to 5000 dollars. Some countries have waivers or discounts for this fee. Ideally, you should look for a journal with no fees. However, keep in mind that most journals with no fees don’t accept case reports while those that accept case reports charge high article processing fees (APCs).
How long does it take to write a Case Report?
The writing part shouldn’t take more than a few days. However, it might take months from the time you submit the article until it gets accepted and additional months from the time it is accepted until it gets published.
Do I need to do a systematic review to publish a case report?
No! Systematic reviews are usually beyond the scope of case reports. However, some case reports may benefit from “brief reviews” in which a non-systematic or standardized search is performed trying to identify all similar cases. If you’re following this guide, probably you performed the literature search prior to starting your case write up and you can include your findings as a summary table.
How long does it take to publish a Case Report?
Like with every other type of publication, the peer-review process and looking around for different journals may take anywhere between months to years. Some journals advertise their time to first decision if you’re in a rush.
Do I need an attending to write a Case Report?
Strictly speaking, no. Some journals have limitations on how many authors can be listed on a case report. However, it’s always a good idea to involve a knowledgeable attending as a senior author to provide expertise on the topic as well as it being a great opportunity to consolidate relationships and network.
Do I need written consent to publish a Case Report?
Consent is required by CARE guidelines and is something you should seek. Some journals have specific consent forms that they require to be submitted with the case. However, the ultimate decision of whether you need a consent will depend on your institution (sometimes case reports with no identifiers and face pictures might not require a consent).
Do I need IRB approval to publish a Case Report?
While the answer may vary between institutions, generally you don’t need an IRB for a case report.
Do I need to know statistics to write a Case Report?
No! If you have a case series you can use descriptive statistics (mean, frequency) which are very easy to do in excel and do not require prior knowledge. If you wish to expand your statistic knowledge, be sure to check out our course on introduction and advanced statistics.
Are case Reports good for my CV?
Yes! Any sort of scholarly activity, especially if published in a well-regarded or indexed journal is a good thing to bolster your application. Having publications by itself is not a requirement per se but helps you show academic inclination and commitment to projects which are attractive to programs. Case reports are a great initial step into research and also make for great components of the CV application. If you wish to expand your research statistic knowledge, be sure to check out our Research and Statistics Courses.
That’s it! Hopefully with this info you’ll be well on your way to writing your first case report. Case reports are a great start to any publishing career and are also a great way to learn about scientific writing and interesting diseases. My own journey to publications started with a couple of case reports and now I have over 40 publications of all types!
By David Hinojosa, MD
David E. Hinojosa-Gonzalez obtained his M.D. from Tecnológico de Monterrey, Mexico in 2020 and led the Surgical Research Outcomes Group for 2 years before joining Massachusetts General Hospital/Harvard Medical School as a Research Fellow in 2021. During this time, he has accumulated over 90 presentations, abstracts, and publications.
Latest Articles
2026 Residency Personal Statement The Ultimate Guide to Crafting Your Residency Personal Statement
Malke Asaad
July 8, 2024

Best Resources for USMLE STEP 1! How to Study and Prepare for STEP1?
Malke Asaad
August 12, 2022
ERAS Application 2026 Guide! How to Fill Out ERAS Residency Application?
Malke Asaad
July 13, 2023
Need Help?
How to find research positions in the US
This live and interactive session + recorded lessons will go over the details of finding research positions in the US.
CV Editing
Our editing goes beyond language and grammar corrections to structural editing and content advising based on your personal story and achievement.
Interview Preparation
The best way to learn something is to do it. That’s why we divide our one-hour interview preparation sessions into two parts. The first half of the session would be a mock interview as if you are interviewing with a program while the second half would provide you with feedback on your performance.
Comprehensive Research Advising
We help advise you on how to find a research position, how to do research, how to make the best use of your research year, how to navigate a research fellowship position, and how to be productive.
USMLE Tutoring
Get personalized study plan and schedule, study resources, and subject-specific tutoring to ace your USMLE exam!
Personal Statement Editing
Our editing includes not only language but also context, structure, and content advising.
ERAS & Supplemental CV
The editing goes beyond language and grammar corrections to structure, design, and content advising based on your personal story and achievement.
Interview Preparation
The best way to learn something is to do it. That’s why we divide our interview preparation sessions into two parts:
Mock Interview + Feedback

Residency
Advising
We are able to provide you with the guidance you need at any step of your journey to make it to your final goal!

{kind=link}
{kind=link}
{kind=link}