
USMLE Blog
USMLE Step 1 High‐Yield Pathology Topics

I hope you enjoy reading this blog post.
If you want our team’s expert help with your USMLE prep, click here
General Pathology
High Yield USMLE Step 1 Notes
Welcome to the General Pathology High-Yield Notes for Step 1.
These are the most commonly tested topics on the exam—ideal for quick review in your last 2 weeks before the exam, when you’re short on time, or when you’re just starting out and want to focus on what is high yield. Created and peer-reviewed by physicians who scored 260+ on Step 1 in a Q&A style to reinforce active learning.
How to use this file
- Read the question ➔ cover the answer ➔ self-quiz before revealing.
- Review the NOTES ➔ they include high-yield details you don’t want to miss.
- Need tutoring? The Match Guy USMLE Tutoring.
- Don’t forget to watch the video lessons that go with this file. Learn more here.
Table of Contents
Cell injury
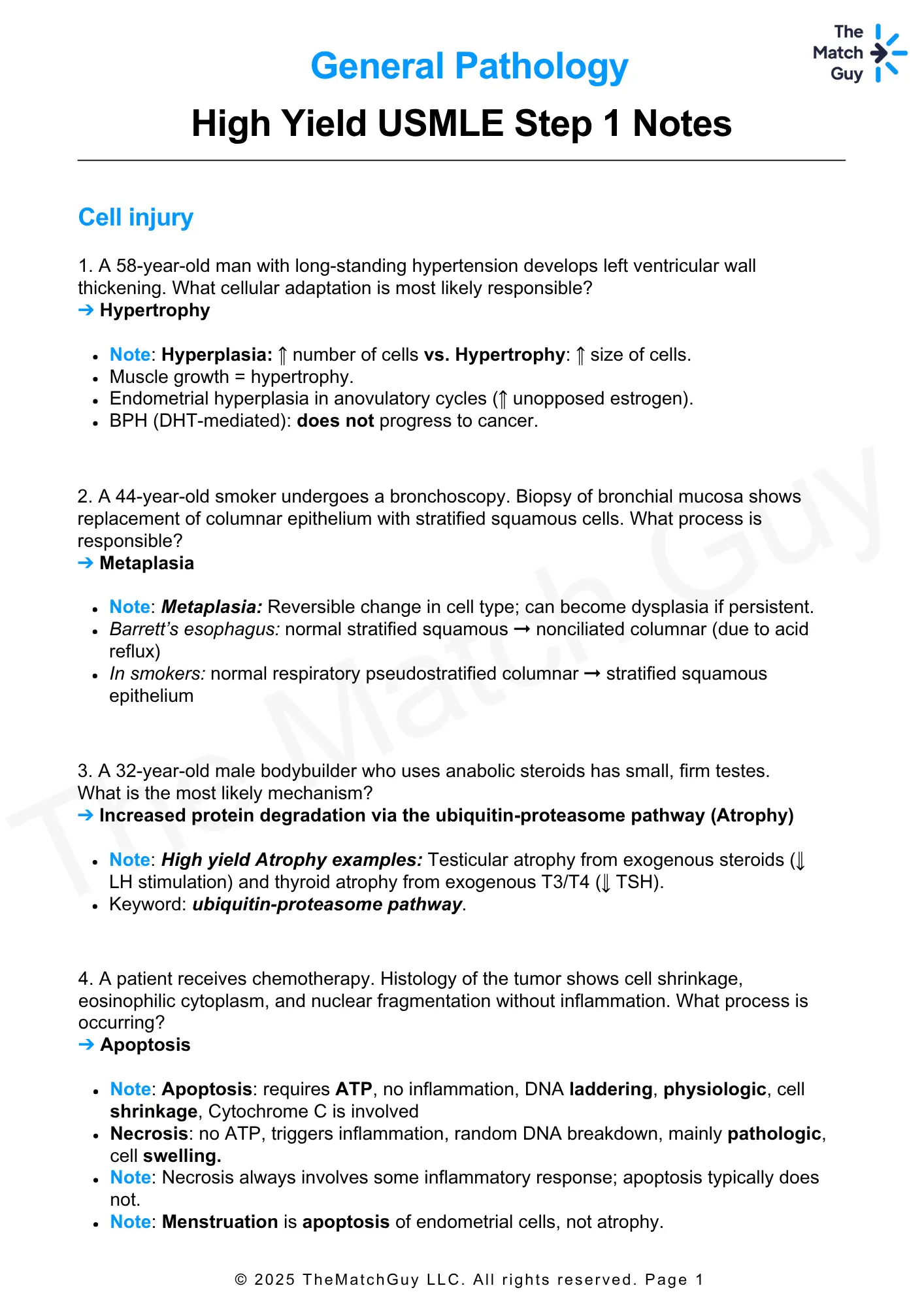
1. A 58-year-old man with long-standing hypertension develops left ventricular wall thickening. What cellular adaptation is most likely responsible?
➔ Hypertrophy
- Note: Hyperplasia: ↑ number of cells vs. Hypertrophy: ↑ size of cells.
- Muscle growth = hypertrophy.
- Endometrial hyperplasia in anovulatory cycles (↑ unopposed estrogen).
- BPH (DHT-mediated): does not progress to cancer.
2. A 44-year-old smoker undergoes a bronchoscopy. Biopsy of bronchial mucosa shows replacement of columnar epithelium with stratified squamous cells. What process is responsible?
➔ Metaplasia
- Note: Metaplasia: Reversible change in cell type; can become dysplasia if persistent.
- Barrett’s esophagus: normal stratified squamous → nonciliated columnar (due to acid reflux)
- In smokers: normal respiratory pseudostratified columnar → stratified squamous epithelium
3. A 32-year-old male bodybuilder who uses anabolic steroids has small, firm testes. What is the most likely mechanism?
➔ Increased protein degradation via the ubiquitin-proteasome pathway (Atrophy)
- Note: High yield Atrophy examples: Testicular atrophy from exogenous steroids (↓ LH stimulation) and thyroid atrophy from exogenous T3/T4 (↓ TSH).
- Keyword: ubiquitin-proteasome pathway.
4. A patient receives chemotherapy. Histology of the tumor shows cell shrinkage, eosinophilic cytoplasm, and nuclear fragmentation without inflammation. What process is occurring?
➔ Apoptosis
- Note: Apoptosis: requires ATP, no inflammation, DNA laddering, physiologic, cell shrinkage, Cytochrome C is involved
- Necrosis: no ATP, triggers inflammation, random DNA breakdown, mainly pathologic, cell swelling.
- Note: Necrosis always involves some inflammatory response; apoptosis typically does not.
- Note: Menstruation is apoptosis of endometrial cells, not atrophy.
5. A patient with acute pancreatitis. Abdominal CT scan shows hyperdense deposits around the pancreas. Caused this?
➔ Saponification of fat tissue (Fat necrosis)
- Note: Fat necrosis can be enzymatic (peripancreatic fat in pancreatitis) or traumatic (e.g., breast tissue). Both have a chalky‐white appearance with saponification.
- Pancreatic parenchyma undergoes liquefactive necrosis in acute pancreatitis.
Prefer learning from crisp, printable PDFs?
Unlock the Entire High-Yield PDF Library — For FREE!
6. A patient develops a black toe with dead tissue. What type of necrosis is involved?
➔ Dry gangrenous necrosis
- Note: Gangrenous necrosis:
- Dry = predominantly coagulative from ischemia (e.g., Peripheral arterial disease (PAD), Frostbite)
- Wet = superinfected → liquefactive overlay (Diabetic foot infections, Bowel infection)
7. A 67-year-old man dies weeks after an ischemic stroke. Brain autopsy shows cystic lesions filled with debris. What best explains the pathogenesis?
➔ Lysosomal enzyme-mediated liquefactive necrosis
- Note: CNS: ischemic infarction → red neurons (eosinophilic), necrosis → Liquefactive necrosis (lysosomal enzymes), scar formation → gliosis (Astrocytes)
Ace Your Step 1 with Expert Guidance.
Struggling with Step 1 preparation? Get personalized 1-on-1 coaching from top scorers and experienced tutors.
Amyloidosis
8. A 70-year-old man with multiple myeloma develops restrictive cardiomyopathy. Biopsy shows apple-green birefringence with Congo red stain. What is the type of amyloid?
➔ AL (amyloid light chain)
- Note: Amyloidosis: Extracellular misfolded β‐pleated sheet proteins.
- Keyword: Congo red stain: apple‐green birefringence.
Primary (AL) vs. secondary (AA) is a classic test distinction.
○ Primary (AL): Ig light chains associated with plasma cell dyscrasias (multiple myeloma).
○ Secondary (AA): serum Amyloid A; seen in chronic inflammatory conditions (e.g., rheumatoid arthritis, IBD).
9. An ESRD patient presents with numbness and tingling in the left hand. Symptoms worsen at night. What is the cause?
➔ Deposition of β₂‐microglobulin (This is a case of carpal tunnel syndrome. It is common in ESRD patients because of Dialysis‐related amyloidosis)
- Note: Special systemic amyloidosis:
- Dialysis‐related: β₂‐microglobulin deposits.
○ Common in long-term ESRD patients.
○ Key: Scapulohumeral arthritis or carpal tunnel syndrome in an ESRD patient. - Age-related: Transthyretin (ATTR) deposition.
- Can be sporadic (elderly, mainly cardiac involvement, benign) or hereditary (familial amyloid polyneuropathies, restrictive cardiomyopathy).
- Key in biopsy of myocardium: ↑ LV wall thickness + pink deposits + ↓ cardiomyocytes.
- Key in clinical vignette: Cardiomyopathy (heart failure) + ↑ LV wall thickness in echocardiography
Inflammation
10. An asymptomatic patient has a positive PPD test and a cavitary lesion in the upper lobe of the right lung. Blocking which cytokine will result in activation of tuberculosis?
➔ Interferon-gamma (IFN-γ)
- Note: Granulomatous Inflammation (A pattern of chronic inflammation).
Activated macrophages (epithelioid histiocytes), sometimes with multinucleated giant cells, surrounded by lymphocytes.
1. Macrophages present antigen to CD4+ T cells → secrete IL‐12 → Th1 differentiation.
2. Th1 cells secrete IFN‐γ → macrophage activation.
3. Activated macrophages (epithelioid) secrete TNF → granuloma maintenance. - Caseating granulomas (central necrosis): almost always infectious
- Noncaseating granulomas (no central necrosis): almost always non-infectious
- Note: Always test for latent TB before starting anti‐TNF therapy (infliximab, adalimumab) → can reactivate TB by breaking down granulomas.
11. A mouse model has deleted ICAM genes. What step of leukocyte extravasation will be impaired?
➔ Tight adhesion
- Note: Leukocyte Extravasation
1. Margination & Rolling – Mediated by selectins (E‐selectin, P‐selectin on endothelium; sialyl‐Lewis on leukocytes).
2. Adhesion (Tight binding) – Integrins (CD18/LFA-1, Mac-1) on leukocytes bind ICAM/VCAM on endothelium.
3. Diapedesis (Transmigration) – Leukocytes cross the endothelium via PECAM‐1 (CD31) at postcapillary venules.
4. Migration (Chemotaxis) – mediated by C5a, IL‐8, LTB4, and bacterial products.
12. A patient with longstanding rheumatoid arthritis presents with microcytic anemia and elevated ferritin. Which molecule is responsible for decreased iron availability?
➔ Hepcidin (acute-phase reactant, ↓ iron absorption → anemia of chronic disease)
- Note: Acute‐Phase Reactants (produced by the liver, upregulated by IL‐6):
- C‐reactive protein (Opsonin)
- Ferritin (inhibit bacterial iron scavenging)
- Fibrinogen (Promotes endothelial repair)
- Hepcidin: Decreases iron release (↓ ferroportin activity) → anemia of chronic disease
- Serum amyloid A (secondary amyloidosis in chronic inflammation).
13. A wound biopsy taken one week after injury shows numerous new capillaries and fibroblast proliferation. Which growth factor is responsible for angiogenesis?
➔ VEGF (vascular endothelial growth factor, promotes new vessel formation, essential for granulation tissue and wound healing.)
- Note: Cytokines and Growth Factors
- IL‐1, IL‐6, TNF‐α: Fever, acute‐phase reactants, endothelial activation.
- IL‐8, LTB4, C5a: Major chemotactic factor for neutrophils.
- TGF‐β: Fibrosis (stimulates collagen deposition), dampens inflammation.
- PDGF: Recruits smooth muscle cells and promotes fibroblast growth.
- VEGF: angiogenesis.
- FGF: angiogenesis, fibroblast proliferation, collagen synthesis, and tissue remodeling.
- IFN‐γ: Activates macrophages and upregulates MHC expression.
- Note: IL-8 contributes to pus formation.
Neoplasia & Oncogenes
14. A 45-year-old woman has a breast mass. Biopsy reveals well-differentiated cells with no mitotic figures and no basement membrane invasion. What type of tumor is this?
➔ Benign tumor
- Note: In the USMLE, despite the location of a mass, you should be able to detect keywords for a benign or malignant tumor.
- Benign: Well‐differentiated, slow‐growing, noninvasive, has no metastases, and moves easily.
- Malignant: Poorly differentiated (anaplastic), erratic growth, local invasion, metastasis, and attached to the surrounding tissue.
15. A patient with gastric adenocarcinoma shows loss of E-cadherin on tumor staining. What is the role of E-cadherin?
➔ Maintains cell–cell adhesion and prevents tumor invasion
- Note: Tumor Spread by:
- ↓ E‐cadherin: Loss of cell‐cell contact.
- ↑ Collagenases: Ability to invade the basement membrane.
16. A 7-year-old boy presents with a rapidly enlarging jaw mass. Biopsy reveals a starry-sky pattern. What oncogene is activated?
➔ c-MYC (Burkitt lymphoma, translocation (8;14)
- Note: High yield Oncogenes (Gain of Function)
- MYC: (c‐myc [t(8;14)] → Burkitt lymphoma)
- BCR‐ABL [t(9;22)]: CML, ALL
- HER2/neu (ERBB2): (breast, gastric carcinoma). It’s a receptor tyrosine kinase.
- RAS: colon, lung, pancreatic
- BRAF: melanoma
17. A young woman is diagnosed with breast cancer. Her mother died from ovarian cancer. What tumor suppressor gene is most likely mutated?
➔ BRCA1 or BRCA2
- Note: Tumor Suppressor Genes (Loss of Function)
- TP53: Li‐Fraumeni syndrome (SBLA syndrome): Sarcoma, Breast, brain, Leukemia, Adrenal.
- RB: retinoblastoma, osteosarcoma
- APC: FAP → colon cancer
- BRCA1/BRCA2: breast, ovarian, pancreatic
- VHL: von Hippel‐Lindau disease, renal cell carcinoma
- WT1: Wilms tumor
18. A patient presents with muscle weakness that improves with activity. Antibodies are found against presynaptic calcium channels. What is the next best step in management?
➔ Chest CT scan
- Note: Paraneoplastic Syndromes:
- Small Cell Lung Cancer:
○ SIADH (↑ ADH) → hyponatremia
○ Cushing Syndrome (↑ ACTH) → hypercortisolism
○ Lambert‐Eaton syndrome (Antibodies against presynaptic Ca²⁺ channels) - Squamous Cell Carcinoma of Lung and renal cell carcinoma:
○ PTHrP → hypercalcemia - Renal Cell Carcinoma, Hemangioblastoma, Hepatocellular carcinoma:
○ ↑ Erythropoietin → polycythemia - Thymoma:
○ Myasthenia Gravis (antibodies against postsynaptic AChRs)
19. A 62-year-old man with a history of shipyard work presents with pleural effusion and dyspnea. Imaging shows pleural thickening. What is the most likely exposure?
➔ Asbestos (mesothelioma)
- Note: Carcinogens
- Asbestos: Lung cancer (bronchogenic >> mesothelioma)
- Aflatoxin (Aspergillus): Hepatocellular carcinoma. Causes DNA damage
- Amatoxin (Amanita Phalloides Mushroom): Liver injury. Affect RNA polymerase II → Block mRNA.
- Vinyl Chloride (PVC pipes): Angiosarcoma of the liver
- Nitrosamines (smoked foods): Gastric carcinoma (intestinal type)
- Ionizing Radiation: Leukemia, papillary thyroid carcinoma
20. A 14-year-old boy has a jaw mass. Biopsy shows a starry-sky appearance. Which virus is involved?
➔ EBV (A case of Burkitt lymphoma, Associated with EBV)
- Note: Oncogenic Microbes
- EBV: Burkitt lymphoma, Hodgkin lymphoma, nasopharyngeal carcinoma
- HPV (16, 18): Cervical, anal, penile, and head/neck cancers.
○ E6 and E7 proteins inactivate the P53 and RB tumor suppressor genes. - H. pylori: Gastric adenocarcinoma, MALT lymphoma
- HBV, HCV: Hepatocellular carcinoma
21. A woman presents with abdominal distension and a pelvic mass. Her CA-125 level is elevated. What is the most likely diagnosis?
➔ Ovarian carcinoma (CA-125 = ovarian carcinoma)
- Note: Tumor Markers: (Mainly used for monitoring rather than diagnosis.)
- AFP: Hepatocellular carcinoma, yolk sac (endodermal sinus) tumors
- β‐hCG: Choriocarcinoma, hydatidiform moles, testicular cancer
- CA‐125: Ovarian carcinoma
- CA 19‐9: Pancreatic adenocarcinoma
- CEA: Colorectal, pancreatic (very nonspecific)
- PSA: Prostate cancer (also ↑ in BPH, prostatitis)
- Calcitonin: Medullary thyroid carcinoma
- Alkaline Phosphatase: Bone metastases, Paget’s disease of bone
🏁 Final Thoughts
You made it to the end—well done! These high-yield notes are designed to save you time and keep you focused on what actually matters for Step 1. Review these vignettes regularly—steady practice beats cramming.
Need one-on-one tutoring? Visit The Match Guy USMLE Tutoring — we’ve helped hundreds of students reach their score goals.
Don’t forget to watch the video lessons that go with this file. They are part of our 7-day high-yield review of Step 1.
Join this RISK FREE live bootcamp 👉 Sign up here
Good luck and we’re rooting for you all the way to Match Day! 🎯
Disclaimer
Version 1.0 May 2025. No part of this document may be reproduced or distributed without written permission. For personal study only. Medical information herein is for educational purposes and does not constitute clinical advice. Always confirm with current guidelines and your institution’s policies.
Prefer a narrative review instead of Q&A style? Scroll down to the section below for high-yield concepts in paragraph format (they cover the same concepts).
Narrative Format
High-Yield Pathology Topics
High‐yield facts on General Pathology that most frequently appear on the USMLE Step 1. Focus on these key associations, mechanisms, and definitions as they are repeatedly tested.
Table of Contents
- Cell Injury
○ Adaptive Responses
○ Apoptosis-vs-Necrosis
○ Amyloidosis - Inflammation
○ Cardinal Signs of Inflammation
○ Chronic Inflammation
○ Leukocyte Extravasation
○ Granulomatous Inflammation
○ Cytokines and Growth Factors - Neoplasia
○ Oncogenes
○ Tumor Suppressor Genes
○ Paraneoplastic Syndromes
○ Carcinogens
○ Tumor Markers
○ Oncogenic Microbes
○ Immune Checkpoint
✅ Get Full Access to All High-Yield Concept PDFs – For FREE!
To access all the PDFs of the Step 1 High-Yield concepts, sign up below and we’ll send them to your inbox — completely free.
Cell Injury
Adaptive Responses
Hyperplasia: ↑ number of cells vs. Hypertrophy: ↑ size of cells.
- Endometrial hyperplasia in anovulatory cycles (↑ unopposed estrogen).
- BPH (DHT-mediated): does not progress to cancer
Dysplasia: Cervical intraepithelial neoplasia due to HPV 16&18. It’s not a normal adaptive response.
Metaplasia: Reversible change in cell type; can become dysplasia if persistent.
- Barrett esophagus: normal stratified squamous → nonciliated columnar (due to acid reflux)
- In smokers: normal respiratory pseudostratified columnar → stratified squamous epithelium
How it is tested: A patient has GERD. Esophagus biopsy shows columnar epithelium. Where do we see a similar adaptive response? Bronchial cells in heavy smokers.
Atrophy examples: Testicular atrophy from exogenous steroids (↓ LH stimulation) and thyroid atrophy from exogenous T3/T4 (↓ TSH). Always emphasize the ubiquitin-proteasome pathway.
How it is tested: A 30-year old bodybuilder has small testes on examination. Which of the following best describes the mechanism? Answer: Increased protein degradation via the ubiquitin-proteasome pathway
Aplasia: DiGeorge Syndrome (Aplasia of 3rd & 4th pharyngeal pouches): Missing thymus (immunodeficiency) + parathyroid glands (hypocalcemia) is a classic presentation.
Apoptosis vs Necrosis
Apoptosis: requires ATP, no inflammation, DNA laddering, physiologic, cell shrinkage, Cytochrome C
Necrosis: no ATP, triggers inflammation, random DNA breakdown, mainly pathologic, cell swelling.
Menstruation is apoptosis of endometrial cells, not atrophy.
Viral hepatitis in USMLE vignettes often involves T‐cell–mediated apoptosis of hepatocytes (not direct viral cytopathic necrosis).
How it is tested: The patient has PCOS. Didn’t menstruate for the past 3 months. Now she has heavy bleeding. Which mechanism is responsible? Answer: Apoptosis
A patient receives chemotherapy for a tumor. Biopsy demonstrates signs of apoptosis. Release of which substance from mitochondria initiates this process? Answer: Cytochrome C
Necrosis always involves some degree of inflammatory response; apoptosis typically does not.
DNA laddering in 180 bp fragments is a classic hallmark of apoptosis.
Fat necrosis can be enzymatic (peripancreatic fat in pancreatitis) or traumatic (e.g., breast tissue). Both have chalky‐white appearance with saponification.
Pancreatic parenchyma undergoes liquefactive necrosis in acute pancreatitis.
Gangrenous necrosis:
Dry = predominantly coagulative from ischemia (e.g., diabetic foot)
Wet = superinfected → liquefactive overlay
CNS: ischemic infarction → red neurons (eosinophilic), necrosis → Liquefactive necrosis (lysosomal enzymes), scar formation → gliosis (Astrocytes)
How it is tested: CVA patient dies. Autopsy shows a cystic cavity inside the brain. What caused that? Answer: Lysosomal enzymes. Or the patient didn’t die. We perform serial biopsies. What would it show? Answer: Glial cell hyperplasia.
Reversible cell injury: cell swelling (earliest), ↓ ATP, membrane blebbing.
Irreversible cell injury: Membrane damage (earliest), mitochondrial dysfunction, nuclear change, rupture of lysosomes.
How it is tested: A patient has an MI. Which of the following is a surrogate for irreversible injury? Answer: Mitochondrial dysfunction
Amyloidosis
Extracellular misfolded β‐pleated sheet proteins.
Congo red stain: apple‐green birefringence = amyloid. Primary (AL) vs. secondary (AA) is a classic test distinction.
Systemic (Generalized) Amyloidosis:
o Primary (AL): Ig light chains associated with plasma cell dyscrasias (e.g., multiple myeloma).
o Secondary (AA): from serum Amyloid A; seen in chronic inflammatory conditions (e.g., rheumatoid arthritis, IBD).
o Transthyretin: can be sporadic (elderly, mainly cardiac involvement, benign) or hereditary (familial amyloid polyneuropathies, restrictive cardiomyopathy).
o Dialysis‐related: β₂‐microglobulin deposits (common in long-term ESRD patients).
How it is tested: A patient has nephrotic syndrome. Kidney biopsy with Congo red stain shows apple-green birefringence. What’s the next step? Answer: The patient has Amyloidosis. The next step is serum protein electrophoresis to detect amyloid A (Plasma cell dyscrasia).
An ESRD patient receives dialysis. Now, she is being evaluated for carpal tunnel syndrome. What’s the mechanism? Answer: Deposition of β₂‐microglobulin.
Inflammation
Cardinal Signs of Inflammation
(Remember the mediators)
Rubor (redness): Vasodilation (histamine, prostaglandins, bradykinin, and NO).
Calor (heat): Increased blood flow and metabolic activity.
Tumor (swelling): Increased vascular permeability → leakage of exudate.
Dolor (pain): prostaglandins (PGE2), bradykinin, histamine.
Functio laesa (loss of function)
Acute Inflammation: Neutrophils
Chronic Inflammation
Mononuclear cells (macrophages, lymphocytes, plasma cells).
Remember this exception: Both acute and chronic transplant rejections are mediated by T-cells. Because both acute and chronic transplant rejections are forms of chronic inflammation.
(Cytokines below are very high yield)
Neutrophils: “First responders”; phagocytose pathogens, cell debris.
Macrophages: Arrive after ~2–3 days; can persist for longer durations in chronic inflammation.
Secrete cytokines (IL‐1, TNF‐α, IL‐6) and growth factors (TGF‐β, PDGF, VEGF)
Present antigens to T cells, promoting adaptive immunity.
Lymphocytes:
T cells secrete cytokines (e.g., IFN‐γ) that activate macrophages.
B cells can differentiate into plasma cells that produce antibodies.
Eosinophils
Parasitic infections and allergic (type I hypersensitivity) reactions. Release Major Basic Proteins (MBP).
Mast Cells/Basophils
Release histamine and are important in allergic reactions and acute inflammatory responses.
How it is tested: Patient with abdominal pain and diarrhea. Stool sample shows Strongyloides stercoralis infection. Which immune cell is most responsible for response? Answer: Eosinophils. Or what would we see on CBC? Answer: Eosinophilia.
Patient with wheezing, hypotension, and urticaria (anaphylaxis). Which cell is responsible? Mast cells.
Leukocyte Extravasation
Margination & Rolling – Mediated by selectins (E‐selectin, P‐selectin on endothelium; sialyl‐Lewis on leukocytes).
Adhesion (Tight binding) – Integrins (CD18/LFA-1, Mac-1) on leukocytes bind ICAM/VCAM on endothelium.
Diapedesis (Transmigration) – Leukocytes cross the endothelium via PECAM‐1 (CD31) at postcapillary venules.
Migration (Chemotaxis) – mediated by C5a, IL‐8, LTB4, and bacterial products.
How it is tested: A rabbit with deleted ICAM gene. Which function is affected? Answer: Tight Adhesion. Remember, selectins, ICAM/VCAM, and PECAM are on the endothelium. Integrins are on leukocytes.
A child is presented with recurrent bacterial infection, delayed umbilical cord separation, and leukocytosis(WBC = 35,000). Examination reveals no pus formation at the infection site. Flow cytometry shows absent CD18 on leukocytes. Which step is impaired? Answer: Adhesion.
Acute‐Phase Reactants (produced by the liver, upregulated by IL‐6)
C‐reactive protein (Opsonin), Ferritin (inhibit bacterial iron scavenging), Fibrinogen (Promotes endothelial repair), Hepcidin: Decreases iron release (↓ ferroportin activity) → can cause anemia of chronic disease, Serum amyloid A (secondary amyloidosis).
How it is tested: A patient with RA presents with microcytic anemia. Ferritin is elevated (an acute-phase reactant, rules out iron deficiency). Which molecule is responsible for anemia? Answer: Hepcidin. Or which interleukin is responsible? Answer: IL-6 (Upregulates the acute-phase reactants)
Granulomatous Inflammation
(A pattern of chronic inflammation).
Activated macrophages (epithelioid histiocytes), sometimes with multinucleated giant cells, surrounded by lymphocytes.
- Macrophages present antigen to CD4+ T cells → secrete IL‐12 → Th1 differentiation.
- Th1 cells secrete IFN‐γ → macrophage activation.
- Activated macrophages (epithelioid) secrete TNF → granuloma maintenance.
- Caseating granulomas (central necrosis): almost always infectious
- Noncaseating granulomas (no central necrosis): almost always non-infectious
High‐yield point: Always test for latent TB before starting anti‐TNF therapy (infliximab, adalimumab) → can reactivate TB by breaking down granulomas.
How it is tested: A patient with signs of chronic pneumonia undergoes a biopsy. Biopsy shows multinucleated giant cells and epithelioid histiocytes. They can ask different questions, like:
Which cells are primarily involved? Answer: Macrophages and CD4+ T Lymphocytes.
What activates the macrophages? Answer: IFN‐γ from Th1 cells.
What activates CD4+ T cells? Answer: Antigen presented by macrophages
The order of migration to the site of inflammation in granuloma is:
Neutrophils → Macrophages(Monocytes) → Lymphocytes.
Cytokines and Growth Factors
IL‐1, IL‐6, TNF‐α: Fever, acute‐phase reactants, endothelial activation.
IL‐8,LTB4,C5a: Major chemotactic factor for neutrophils.
TGF‐β: Fibrosis (stimulates collagen deposition), dampens inflammation.
PDGF: Recruits smooth muscle cells and promotes fibroblast growth.
VEGF: Stimulates angiogenesis.
FGF: Stimulates, angiogenesis, fibroblast proliferation, collagen synthesis, and tissue remodeling.
IFN‐γ: Activates macrophages and upregulates MHC expression.
How it is tested: A scenario for wound infection. Which molecule is responsible for pus? Answer: IL-8; Or a new wound biopsy is shown. The biopsy shows granulation tissue with a lot of capillaries. Which one is responsible for the angiogenesis? Answer: VEGF
Neoplasia
Benign: Well‐differentiated, slow‐growing, noninvasive, no metastases.
Malignant: Poorly differentiated (anaplastic), erratic growth, local invasion, metastasis.
↓ E‐cadherin: Loss of cell‐cell contact
↑ Collagenases: Ability to invade basement membrane.
Blood or lymphatic invasion: Ability to spread.
How it is tested: A woman presents with a slow-growing breast mass. Biopsy shows well-differentiated ductal epithelial cells with intact basement membrane and no evidence of mitotic figures. Which of the following best describes this lesion? Answer: Benign tumor.
A patient with gastric adenocarcinoma. Genetic testing of the tumor shows loss of E-cadherin expression. What’s the mechanism of tumor spread? Answer: Loss of cell-cell adhesion
Oncogenes
(Gain of Function)
They may give you one cancer, and ask about the risk of other cancers based on the gene involved.
MYC: (c‐myc [t(8;14)] → Burkitt lymphoma)
BCR‐ABL [t(9;22)]: CML, ALL
HER2/neu (ERBB2): (breast, gastric carcinoma). It’s a receptor tyrosine kinase.
RAS: colon, lung, pancreatic
BRAF: melanoma
Tumor Suppressor Genes
(Loss of Function)
TP53: Li‐Fraumeni syndrome (SBLA syndrome): =Sarcoma, Breast, brain, Leukemia, Adrenal.
RB: retinoblastoma, osteosarcoma
APC: FAP → colon cancer
BRCA1/BRCA2: breast, ovarian, pancreatic
VHL: von Hippel‐Lindau disease, renal cell carcinoma
WT1: Wilms tumor
How it is tested: A patient presents with fatigue, night sweats, and splenomegaly. Blood smear shows increased neutrophils, basophilia, and myelocytes. Genetic testing reveals a t(9;22) translocation. What’s the diagnosis? CML.
A woman presents with a sarcoma in her thigh. Her mother had breast cancer at age 30, and her uncle died of brain cancer at 35 (she has Li-Fraumeni syndrome). Which other malignancy is she at increased risk for? Answer: Adrenal Carcinoma
A patient with a family history of colorectal cancer has numerous adenomatous polyps throughout his colon. Which gene? APC. Risk of cancer? 100%. Treatment? Prophylactic colectomy.
Paraneoplastic Syndromes
(A classic question will show you paraneoplastic syndrome and will ask you other questions about cancer. For example, if the patient has Lambert-Eaton, the next step is a Chest CT scan to find the tumor. Or if the patient has thymoma, you should know this can cause MG)
Small Cell Lung Cancer: originated from neurons and have paraneoplastic syndromes related to neuronal function.
SIADH (↑ ADH) → hyponatremia
Cushing Syndrome (↑ ACTH) → hypercortisolism
Lambert‐Eaton syndrome (Antibodies against presynaptic Ca²⁺ channels)
Squamous Cell Carcinoma of Lung:
PTHrP → hypercalcemia
Renal Cell Carcinoma, Hemangioblastoma, Hepatocellular carcinoma:
↑ Erythropoietin → polycythemia
Thymoma:
Myasthenia Gravis (antibodies against postsynaptic AChRs)
How it is tested: A 64-year-old man with a history of heavy smoking presents with confusion, nausea, and muscle cramps. Labs show serum sodium of 118 mEq/L. What’s the most likely cause of this patient’s symptoms? Answer: Excessive ADH secretion (SIADH).
USMLE will present to you a patient with neuromuscular junction disorder. You should be able to differentiate between lambert-eaton myasthenic syndrome(LEMS) and myasthenia gravis (MG). If it’s lambert-eaton, take a chest CT scan to look for small cell lung cancer. If it’s Myasthenia gravis, also take a chest CT scan to look for thymoma. They can also ask: What kind of antibody is produced? (In case you have issues with differentiating these two, check neuro resources.)
Carcinogens
- Asbestos: Lung cancer (bronchogenic >> mesothelioma)
- Aflatoxin (Aspergillus): Hepatocellular carcinoma. Causes DNA damage
- Amatoxin (Amanita Phalloides Mushroom): Liver injury. Affect RNA polymerase II → Block mRNA.
- Vinyl Chloride (PVC pipes): Angiosarcoma of the liver
- Nitrosamines (smoked foods): Gastric carcinoma (intestinal type)
- Ionizing Radiation: Leukemia, papillary thyroid carcinoma
How it is tested: A patient who worked in shipbuilding or insulation presents with progressive shortness of breath. Chest X-ray shows pleural thickening and effusions. What is the most likely exposure? Answer: Asbestos
Tumor Markers
(Mainly used for monitoring rather than diagnosis.)
- AFP: Hepatocellular carcinoma, yolk sac (endodermal sinus) tumors
- β‐hCG: Choriocarcinoma, hydatidiform moles, testicular cancer
- CA‐125: Ovarian carcinoma
- CA 19‐9: Pancreatic adenocarcinoma
- CEA: Colorectal, pancreatic (very nonspecific)
- PSA: Prostate cancer (also ↑ in BPH, prostatitis)
- Calcitonin: Medullary thyroid carcinoma
- Alkaline Phosphatase: Bone metastases, Paget disease of bone
How it is tested: A woman with abdominal bloating, early satiety and weight loss. Imaging: a pelvic mass. Lab tests: elevated CA-125. Diagnosis? Answer: Ovarian carcinoma.
Or elevated β-hCG in men is Choriocarcinoma. So if you see elevated β-hCG in a man, the next step is testicular ultrasound and orchiectomy.
Oncogenic Microbes
- EBV: Burkitt lymphoma, Hodgkin lymphoma, nasopharyngeal carcinoma
- HPV (16, 18): Cervical, anal, penile, and head/neck cancers. E6, E7 inactivates P53, RB tumor suppressor genes.
- H. pylori: Gastric adenocarcinoma, MALT lymphoma
- HBV, HCV: Hepatocellular carcinoma
How it is tested: A 14-year-old boy with a rapidly enlarging jaw mass. Biopsy of the mass shows sheets of lymphocytes with interspersed macrophages, giving a “starry sky” appearance (or genetic testing shows t(8;14) translocation). Which virus is strongly associated? Answer: EBV. (Remember, it’s not CMV. Most students confuse these two viruses.)
A routine Pap smear reveals koilocytic changes (perinuclear halos). HPV testing is positive for HPV-16. What’s the most likely mechanism? Inactivation of P53 and Rb.
A patient presents with epigastric pain and early satiety. Biopsy shows lymphoid tissue with monoclonal B-cell proliferation, and H. pylori is detected. Best initial treatment? Triple therapy (omeprazole, clarithromycin, amoxicillin) to eradicate H.pylori.
Grade = degree of differentiation (well vs. poorly) + mitotic activity.
High‐grade = Poorly differentiated → more aggressive.
Stage = extent of tumor spread (TNM: Tumor size, Nodes, Metastases).
Stage (Metastasis) is the single most prognostic factor NOT grade.
Immune Checkpoint
Tumors upregulate PD‐L1 → bind PD‐1 on T‐cells → T‐cell exhaustion.
Anti–PD‐1 (nivolumab, pembrolizumab) or anti–PD‐L1 (atezolizumab) restore T‐cell activity.
CTLA‐4 on T‐cells outcompetes CD28 → decreased co‐stimulation.
Ipilimumab (anti–CTLA–4) blocks this inhibitory signal.
How it is tested: A 55-year-old man with metastatic melanoma is treated with ipilimumab, a medication that blocks CTLA-4 on T cells. He develops severe colitis and dermatitis. What’s the function of CTLA-4? Answer: it’s upregulated by tumor cells on T cells to outcompetes CD28 binding to B7(CD80/86) on Antigen presenting cells (APCss)
A 55-year-old man with metastatic melanoma is treated with ipilimumab, but he develops severe colitis and dermatitis. What is the mechanism of action of this drug? Answer: Blocks CTLA-4, enhancing T-cell activation
Ace Your Step 1 with Expert Guidance.
Struggling with Step 1 preparation? Get personalized 1-on-1 coaching from top scorers and experienced mentors.
To access all the PDFs of the Step 1 High-Yield Topics, please sign-up below for free and we will deliver the full PDFs directly to your email inbox!
If you need guidance on your target USMLE scores or have questions on improving your chances of matching into your dream specialty, feel free to schedule a call here or text us on WhatsApp here for personalized support.
🍀 We wish you best of luck on your exam!
Latest Articles
2026 Residency Personal Statement The Ultimate Guide to Crafting Your Residency Personal Statement
Malke Asaad
July 8, 2024

Best Resources for USMLE STEP 1! How to Study and Prepare for STEP1?
Malke Asaad
August 12, 2022
ERAS Application 2026 Guide! How to Fill Out ERAS Residency Application?
Malke Asaad
July 13, 2023
Need Help?
About TheMatchGuy
The Match Guy is a premier medical consulting firm trusted by over 35,000 students worldwide. We help medical students and graduates excel on the USMLE (Step 1, Step 2 CK, and Step 3) and strengthen their residency applications through proven study strategies, expert tutoring, and personalized guidance from elite 260+ scoring tutors who have helped countless students achieve their goals. Whether you’re aiming for a competitive specialty or navigating the Match as an IMG, we help you prepare smarter, avoid burnout, and position yourself as a strong applicant from exam day through Match season. Schedule a FREE discovery call now.
RECOMMENDED ARTICLES
Best Electives in the US

Best Resources for USMLE STEP 1! How to Study and Prepare for STEP1?

United States Clinical Experience for IMGs
